

Introduction
Emicizumab (a bispecific antibody mimicking Factor VIIIa) has been authorised for use in the United Kingdom National Health Service (NHS) in severe hemophilia A patients with and without inhibitors since August 2019. The Summary of Product Characteristics estimates a steady state of emicizumab achieved after four loading doses for patients >12 years of age at between 50-60ug/mL. Real world data outwith trial conditions are lacking to evaluate clinical efficacy, and which assays may be appropriate to determine emicizumab levels in vivo.
Methods
A prospective analysis of patients switching from FVIII concentrate to emicizumab was conducted at Guy's and St Thomas' Hospital Haemophilia Centre between September 2019 and July 2020 inclusive. Patients' age and weight were recorded and doses of emicizumab prescribed according to United Kingdom Haemophilia Centres' Doctors Organisation guidelines. Post emicizumab initiation, samples for coagulation testing were taken one week, four weeks and eight weeks after commencing emicizumab, with some pre-emicizumab initiation samples obtained. Three assays were used (human chromogenic FVIII assay (CSA) (Hyphen Biomed); bovine chromogenic FVIII assay (BCA) (Siemens); and a modified one-stage emicizumab assay (OSEA) with emicizumab calibrators to derive drug levels). Where possible with sufficient sample volume all three assays were run simultaneously.
Results
Within the cohort of all severe hemophilia A patients (n=118), 9 patients with inhibitors had already been previously switched from FVIII concentrate. 21 patients switched to emicizumab between September 2019 and July 2020, of which 2 patients had active FVIII inhibitors, with emicizumab prophylaxis patients comprising 25.4% (30/118) of the hospital cohort. Mean age of switchers was 39.3 years (standard deviation ± 13.9), with a mean dose of 116 ± 20.7mg on a weekly basis. 13/21 were on 1.5mg/kg weekly dosing and the remainder on fortnightly dosing at 3mg/kg.
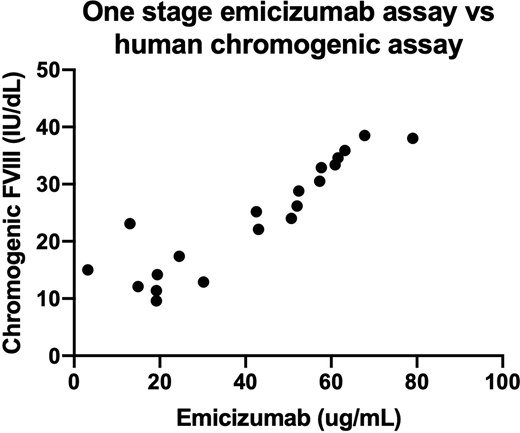
OSEA levels at 1 week (n=15), 4 weeks (n=15) and 8 weeks (n=7) were 19.7 ± 14.8ug/mL, 54.8 ± 11.7ug/mL and 61.3 ± 12.2ug/mL respectively. CSA results were 17 ± 9.0 IU/dL (n=9), 27.7 ± 6.7 IU/dL (n=10), and 26.7 ± 9.6 IU/dL (n=5) respectively. Simultaneous 1-stage based OSEA and CSA assays were performed on 20 samples, with high correlation between the two types of assay (Pearson correlation coefficient = 0.909 (CI 0.780-0.964, p <0.0001)). Six pre-emicizumab initiation samples were tested for both OSEA and CSA, which suggested low-level cross-reactivity of OSEA with FVIII concentrate in vivo. 4/6 were non-washout samples, which showed apparent positive OSEA levels (range 2.3-7.9ug/mL) with corresponding CSA ranges from 17.6-86.6 IU/dL.
BCA in 3 patients at 1 week showed a low level of residual FVIII (all <8 IU/dL) consistent with prior FVIII infusions. All samples at 4 weeks and 8 weeks had undetectable FVIII concentrate levels consistent with the cessation of FVIII administration (bovine FVIII <1 IU/dL) and correspondingly positive OSEA levels, confirming the lack of cross-reactivity between the two assays.
No patients developed anti-emicizumab antibodies as determined by clinical efficacy or by APTT measurement. No patients required any surgical or interventional procedures during this period. One spontaneous bleed and one traumatic bleed were recorded in two separate patients.
Conclusion
Emicizumab in a real-world setting is confirmed in our experience to have excellent clinical efficacy with infrequent episodes of spontaneous bleeding. 18% of patients switched to emicizumab within a year of its availability on the NHS. It has been well-tolerated with no clinical or laboratory evidence of anti-drug antibodies as measured by APTT.
The OSEA correlated well with levels predicted by the emicizumab SPC at each time point. At all concentrations an OSEA and CSA are highly correlated, which may suggest that only one of the two assays is routinely required in laboratory use to assay emicizumab. Caution is however advised in assessing OSEA on its own when FVIII concentrate has recently been administered as this may result in some low level, false positive results.
Austin:Chugai: Honoraria. Dolan:Pfizer: Consultancy; Roche: Honoraria.

